上一期,我们聊了美国急诊医生养成记:「经历这 4 年,才能成为美国急诊科医生」这次让我们谈一谈美国对于急诊科患者的分级诊疗。
来听 Dr.Hou 聊聊……《 中国急诊患者分 4 级,美国为啥分 5 级?》

中美医生介绍
美国医生:侯全益医生,哈佛医学院急诊科讲师, 布列根和妇女医院急诊科医生,外科 ICU 重症监护专家。
U.S. doctor: Dr. Peter Hou is an Instructor in Emergency Medicine at Harvard Medical School, an Emergency Physician at Brigham and Women’s Hospital, and a critical care specialist in the Surgical ICU.
中国医生:宋瑞医生,曾在中国和新加坡担任内科住院医师,现为自由作家,同时在波士顿进行自闭症相关临床研究。
Chinese doctor: Dr. Rui Song, former resident physician of internal medicine in China and Singapore, freelancer and she is doing autism clinical research on Autism in Boston.
Dr. 宋:侯医生,我相信您在急诊科见到过形形色色不同的病例 。但是,从医学的角度来看,患者并不知道自己的状况是多么危急,紧急,还是非紧急。今天我们来谈谈这些不同紧急程度的临床表现好吗?
Dr. Hou, I’m sure you’ve seen a variety of different presentations in the ED. However, patients do not know how emergent, urgent, or not urgent their conditions are from a medical perspective. Today, shall we talk about these presentations?
Dr. 侯:当然可以。
Sure.
Dr. 宋:有些人可能会认为高烧是一种紧急情况。然而,轻微的胸痛可能比那更严重。如今在中国,我们有护士在急诊科进行分诊,在询问病史,进行体格检查和生命体征的测量后,她会根据不同的病情紧急程度进行优先排序。中国有 4 个级别来对患者进行紧急程度分层,那么在美国呢?
Some people may consider high fever as an urgent condition.However, a mild chest pain may be more serious than that. Nowadays in China, we have nurses in the ED triage to prioritize different conditions after taking a focus history, exam, and vital signs.We have 4 levels to stratify patients. How about that in the U.S.?
Dr. 侯:在美国,大多数急诊科使用急诊危重度指数(ESI)来对急诊科患者进行分诊。ESI 是一种五级分类算法,它根据患者的临床问题的紧急程度和所需的预期资源,将患者的临床相关分层分为 1 级(危急)至 5 级(非紧急)。 ESI 中「资源」的概念是指除了体检外的复杂的诊断与干预措施,包括 X 射线、CT、超声、核磁共振、心电图、血液检查、静脉药物、床旁操作和医疗咨询。你是否知道,最初的 ESI 概念「不仅是什么时候应该看这个病人,还有这个病人需要什么?」是由于埃特尔医生和维尔茨医生在 1998 年提出的,其中维尔茨医生是我们布列根和妇女医院的急诊科医师之一?
In the U.S.,most ED’s use the Emergency Severity Index (ESI) to triage patients who present to the ED. ESI is a five-level triage algorithm that provides clinically relevant stratification of patients into levels from 1 (emergent) to 5 (least urgent), based on acuity of patients' health care problems and anticipated resources required.The concept of「resources」in ESI refers to complex diagnostics and interventions in addition to physical examination.Examples of resources include X-ray, CT, Ultrasound, MRI, ECG, blood tests, intravenous medications, bedside procedures, and consultations. Did you know that the original ESI concept of「not only when should this patient be seen, but also what does this patient need?」was developed in 1998 by Drs. Eitel and Wuerz, and Dr. Wuerz was one of our Brigham Emergency Physician?
Dr. 宋:不知道,真有趣呢!请您跟我多讲讲。
No, how interesting! Please tell me more.
Dr. 侯:初步的「新型五级分诊工具的可靠性和有效性」试点研究在布列根和妇女医院和麻省总院的急诊科进行。接下来这个分诊工具在护理实践中实施,ESI 在布列根和妇女医院以及北卡罗莱纳大学的急诊科得到进一步完善。
The initial pilot study of「Reliability and Validity of a New Five-level Triage Instrument」was performed in the EDs at the Brigham and Women’s and Massachusetts General Hospitals. Then it was implemented into nursing practice and ESI was further refined in the EDs at Brigham and Women’s Hospital and University of North Carolina.
Dr. 宋:那么 ESI 的 5 个级别都代表什么呢?
So what does the 5 levels of ESI represent?
Dr. 侯:下面的表格说明了这 5 个级别和病情举例:
This following table represents the 5 levels and for examples:
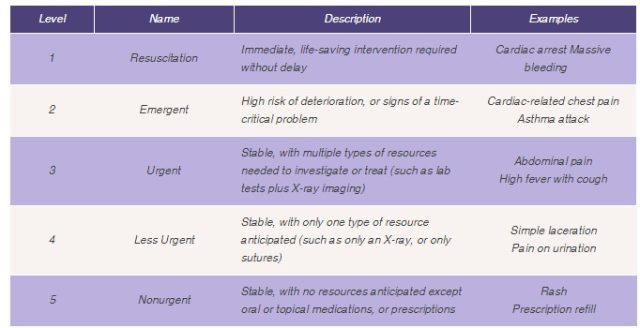
看明白美国 ESI 的 5 个级别都代表什么了么?关注「丁香智汇」,回复关键词「5」,获得中文翻译表~
Dr. 宋:谢谢您的分享。 ESI 充分利用了急诊医疗资源。但是,我有一个问题。对于那些情况不那么紧急的人,如割伤或脚踝扭伤,他们可能需要等待很长时间才能见到急诊科医生。虽然他们的状况并不危急,但他们可能非常痛苦。有没有任何解决方案能让他们得到更快的治疗?
Thank you for your sharing. The ESI makes full use of emergent medical resources to those in need. However, I have a question. For those with less urgent conditions, such as a cut or ankle sprain, they may wait for a long time before being seen by a ED provider. Though their conditions are not emergent, they may suffer greatly. Any solution to minimize their waiting time?
Dr. 侯:是的。我们看到最近有越来越多的紧急护理中心和小型健康诊所正在建立起来,以匹配非危急状况的病人人群。此外,某些州还允许「独立急诊室」的运营。另外,许多医院急诊科正在用远程医师视频会议的方式让高级医疗专家帮助诊治病人。最后,许多医院急诊科还开始实施「按需视频门诊」,使得患者可以随时随地联络到急诊科医生。
Yes. We have seen recently increasing number of urgent care centers and mini-health clinics being built to tailor to patients presenting with non-emergent conditions. In addition, there are「free standing EDs」allowed by certain states. Also, many EDs are incorporating remote physician video conferencing with advance practitioners to help facilitate patient care. Lastly, many EDs are starting to implement「On-Demand Video Visits」in which patients can connect to an emergency physician anytime and anywhere.
Dr. 宋:哇,这真的是急诊科专业领域非常令人兴奋的新创新。它们可能可以缓解非常繁忙的需要很长等待时间的急诊科的拥挤负担。谢谢侯医生今天的节目。下期再见。
Wow, this sounds like very exciting new innovations for the specialty of emergency medicine. That could potentially relief the burden of crowding in very busy EDs with long waiting time. Thank you Dr. Hou for today’s program. See you next time.
下一期讲什么?
what will we talk about?
由你来决定!
如果你是医学英文爱好者,欢迎回复加群,备注:医院+医学英文,加入医学英文爱好者群中,还会有单词小笔记送出!
参考文献
1.https://www.ncbi.nlm.nih.gov/pubmed/10730830
2.https://www.ncbi.nlm.nih.gov/pubmed/11157294
3.https://www.ahrq.gov/professionals/systems/hospital/esi/index.html
4.http://www.esitriage.org/;
5.https://www.esitriage.com/
6.https://catalyst.nejm.org/telehealth-express-care-service-revolutionizing-ed-care/
封面图片来源「shutterstock」
编辑|晓玮
文章转载授权及合作事宜请联系微信「panda_wqy」
扫描下方二维码关注「丁香智汇」,阅读更多精彩文章!

